Stoned Kidneys


SINCE its introduction in the early 80s. the use of shock waves to pulverise kidney stones has become common practice. Doctors have found, though, that the brunt of the treatment can cause short-term damage to surrounding tissues. Might this procedure, called lithotripsy, have long-term effects as well?
A study compared medical data on 288 people who had lithotripsy about 19 years earlier with an equal number whose kidney stones had been treated at the same time in a different, nonsurgical way. Over the ensuing years. 182 people developed hypertension and 67 developed diabetes. Lithotripsy recipients were nearly four times more likely to have diabetes and 50% more apt to have hypertension than were those not exposed to the shock-wave technology. The more shock treatments people received, the higher their risk of diabetes. People who had lithotripsy on both kidneys had a higher risk of hypertension than did those who had one kidney treated.
Who may be affected by these findings? People who have had or are considering lithotripsy. Most kidney stones are small enough to pass through the urinary system on their own; larger stones can be dissolved by medicine, removed surgically, plucked out through a tube threaded through the ureter or smashed via lithotripsy.
Caveats: Newer lithotripters, the machines that deliver the shock waves, have a more narrow focus area and might produce different effects.
You can find this study in the May issue of the Journal Of Urology; abstract available online at www.jurology.com.
Learn more about kidney stones at www.kidney.org and http://kidney.niddk.nih.gov. - LAT-WP
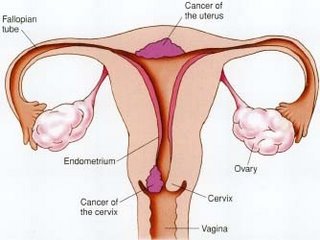
Uterine prolapse and incontinence
WEAKENED pelvic muscles can cause the uterus to sag and sometimes protrude through the vaginal opening, To correct this, women usually have surgery, called sacro- colpopexy. Afterward, however, coughing or sneezing often causes urine leakage. To prevent this so-called stress incontinence, might it help to have an additional procedure at the time of surgery, suturing the vagina to a pelvic ligament?
A study randomly assigned about half of 322 women undergoing sacrocolpopexy to have a second procedure, a Burch colposuspension, at the same time. Three months later, 44% of the women who had Only the surgery reported symptoms of stress incontinence, compared with 24% of those who also had the Burch procedure. About four times more women in the surgery-only
group than in the Burch group reported the most bothersome symptoms.
Who may be affected by.these findings? Women with pelvic organ prolapse, which can occur after frequent childbirth or with
ageing.
Caveats: Surgeries lasted about 12% longer when they included the Butch procedure. Long-term effectiveness remains unknown.
Whether the findings apply to women who have different surgical procedures for prolapse or incontinence remains unclear.
You can find this study in the April 13 issue of the New Engiand Journal of Medicine; abstract available online at www.nejIn.org:r Learn more about uterine prolapse at www.mayoclinic.com and www.medem.com (search for "pelvic support"). - LAT-WP
Mercury in cavities
WHEN children are exposed to even low levels of lead. their 1Q scores have been shown to suffer. Might the same occur with
exposure to another known neurotoxin, mercury, which is contained in the silver, or amalgam, fillings often used to restore teeth damaged by cavities?
A study randomly assigned 534 children, six to 10 years old, to have cavities in their back teeth filled with either amalgam or a mercury-free, resin-based composite material. None of the children had any existing amalgam fillings, and only a few had detectable levels of mercury in their urine. After five years, mercury levels had increased in both groups but were higher in the amalgam group. However. periodic neuropsychological tests (of memory, learning, visual-motor skills) and 1Q scores showed no real differences between the groups.
Who may be affected by these findings? Children of elementary school age. Amalgam fillings have been used for about 150 years; newer composite materials, tooth-coloured but usually more costly, often are used to fill cavities in the more visible front teeth.
Caveats: Findings may not apply to younger children and to others who may be especially sensitive to mercury. The study did not determine whether exposure as a child could lead to negative health effects later in life, and it was not designed to detect whether exposure produced minor effects in children.
You can find this study in the April 19 issue of the Journal of the American Medical Association: abstract available online at www.jama.com. Learn more about cavities at http://kidshealth.org and www.ada.org. - LAT-WP
Note: The research described in Quick Study comes from credible, peer-reviewed journals. Nonetheless, conclusive evidence about a treatrnent's effectiveness is rarely found in a single study. Anyone considering changing or beginning treatment of any kind should consult with a physician.
Labels: Stoned Kidneys, vaginal
posted by Master @ 8:43 AM
0 Comments
Links to this post
![]()
![]()